
Key Takeaways for Recovery
- Early Intervention: Rehab typically starts within 24-72 hours of medical stabilization to prevent secondary complications.
- Recovery Potential: Those with incomplete injuries can often reach 80-90% of their functional potential within the first year.
- Tech Integration: Tools like exoskeletons and FES cycling are shifting the ceiling of what's possible in mobility.
- Holistic Care: Success depends on a multidisciplinary team, including physical therapists, psychologists, and nurses.
Understanding Function Loss and Injury Levels
Not all injuries are the same. The impact depends entirely on where the damage occurred and whether the spinal cord was completely severed or just bruised. In the medical world, we talk about "complete" versus "incomplete" injuries. If an injury is complete, no signals get through. If it's incomplete, some pathways remain open, which significantly changes the prognosis. For example, while only 1-3% of complete paraplegics regain the ability to walk, nearly 59% of those with incomplete injuries do. The level of injury also dictates what functions are lost. Cervical injuries (C1-C4) are the most severe, often affecting the ability to breathe independently and move the arms. At the C5-C6 level, you might regain some shoulder and elbow movement, but you'll still face challenges with grip and hand function. Lower injuries, like those in the thoracic or lumbar regions, typically result in paraplegia, affecting the legs and pelvic organs while leaving the upper body fully functional.The Road to Recovery: Phases of Rehabilitation
Rehab isn't a single event; it's a progression. The clock starts ticking the moment you are medically stable. If you wait too long, you risk muscle atrophy and joint contractures-where your limbs essentially "lock" in place.The Acute Phase (First few weeks): This stage is all about survival and protection. The focus is on respiratory care to prevent pneumonia and passive range of motion (ROM) exercises. If a patient has spasticity (muscle stiffness), these exercises happen 2-3 times a day just to keep the joints moving. It's grueling and repetitive, but it's the foundation for everything that follows.
The Subacute Phase (2-12 weeks): This is where the hard work begins. Patients typically enter an inpatient program involving at least three hours of therapy five days a week. You'll start seeing a team of experts: neuropsychologists to handle the mental toll, occupational therapists for daily living skills, and physical therapists for mobility. This phase introduces active-assisted exercises and the first attempts at wheelchair transfers.
Community Reintegration (3-6 months and beyond): The goal here is to get you back home. Outpatient programs focus on navigating a real-world environment-getting into a car, managing a kitchen, and returning to work. This is also where the mental game becomes critical; peer support programs are vital here, with many patients reporting that talking to someone who has "been there" is the only thing that helps them adjust.
Assistive Devices and High-Tech Interventions
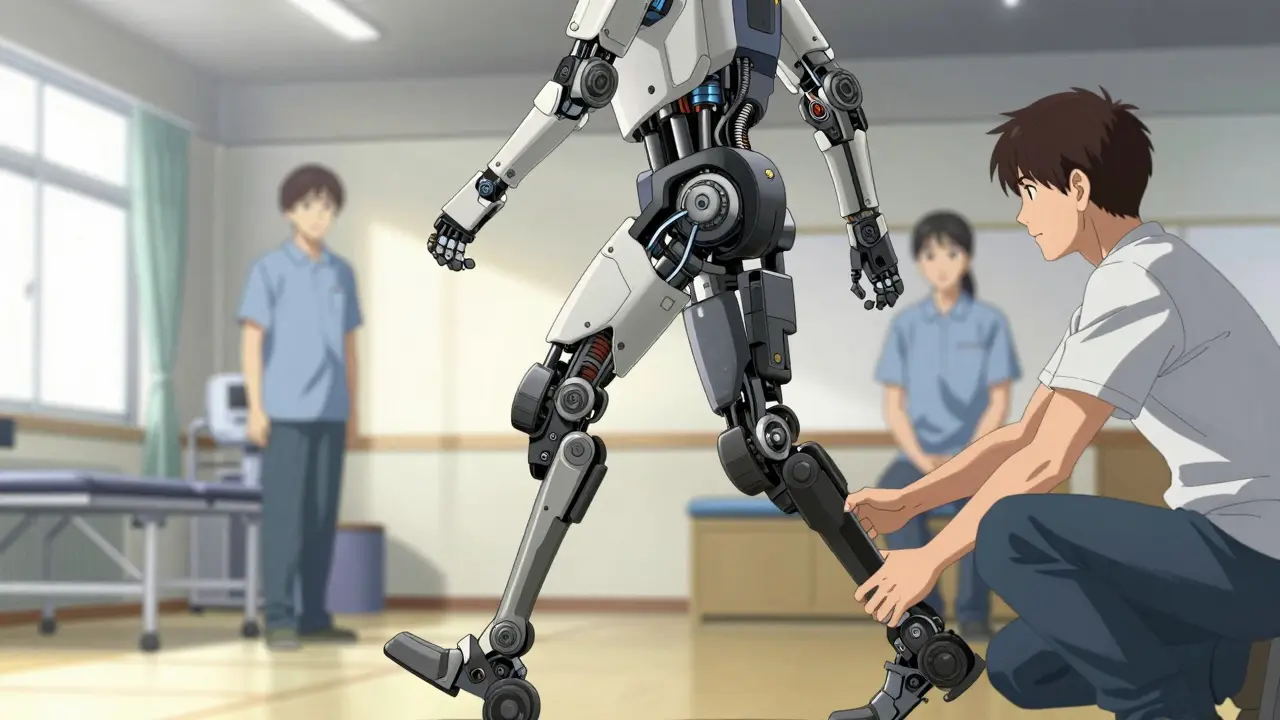
We've come a long way from just using a standard manual wheelchair. Today, technology acts as a bridge for the missing neural connections. Functional Electrical Stimulation (or FES) is a game-changer. By using electrical pulses to trigger muscle contractions, FES cycling helps maintain leg muscle mass and boosts cardiovascular health. In fact, FES cycling can increase peak oxygen consumption by over 14%, which is far more effective than traditional arm cycling. Then there are the "robot suits." Exoskeletons like Ekso and ReWalk allow people with complete paralysis to stand and take steps. While they are incredible for psychological morale and physical health, they aren't perfect. They require a lot of energy and often need 2-3 therapists to operate safely, meaning sessions are usually limited to 30-45 minutes.| Technology | Primary Benefit | Main Limitation | Best For |
|---|---|---|---|
| FES Cycling | Cardiovascular health & muscle mass | High out-of-pocket cost | T-level and L-level injuries |
| Exoskeletons | Upright mobility & bone density | Short session limits (30-45 min) | Paraplegia / Incomplete SCI |
| Body Weight Support | Safe gait training & walking speed | Different walking patterns than natural | Incomplete SCI patients |
| Diaphragm Pacing | Reduced ventilator dependence | Surgical implantation required | C3-C5 high cervical injuries |
Managing the "Invisible" Challenges
When people think of SCI, they think of wheelchairs. But the hardest parts of the day often happen behind closed doors. Neurogenic bowel and bladder management is a relentless task, often requiring 45 to 90 minutes of specialized care every single day. If not managed perfectly, it leads to infections and skin breakdown. Spasticity is another hurdle. It's that sudden, involuntary muscle tightening that can be painful and disruptive. Doctors often use a combination of oral medications like baclofen and targeted botulinum toxin injections to calm the muscles. When done right, this can reduce spasticity scores by 40-60% for the majority of patients.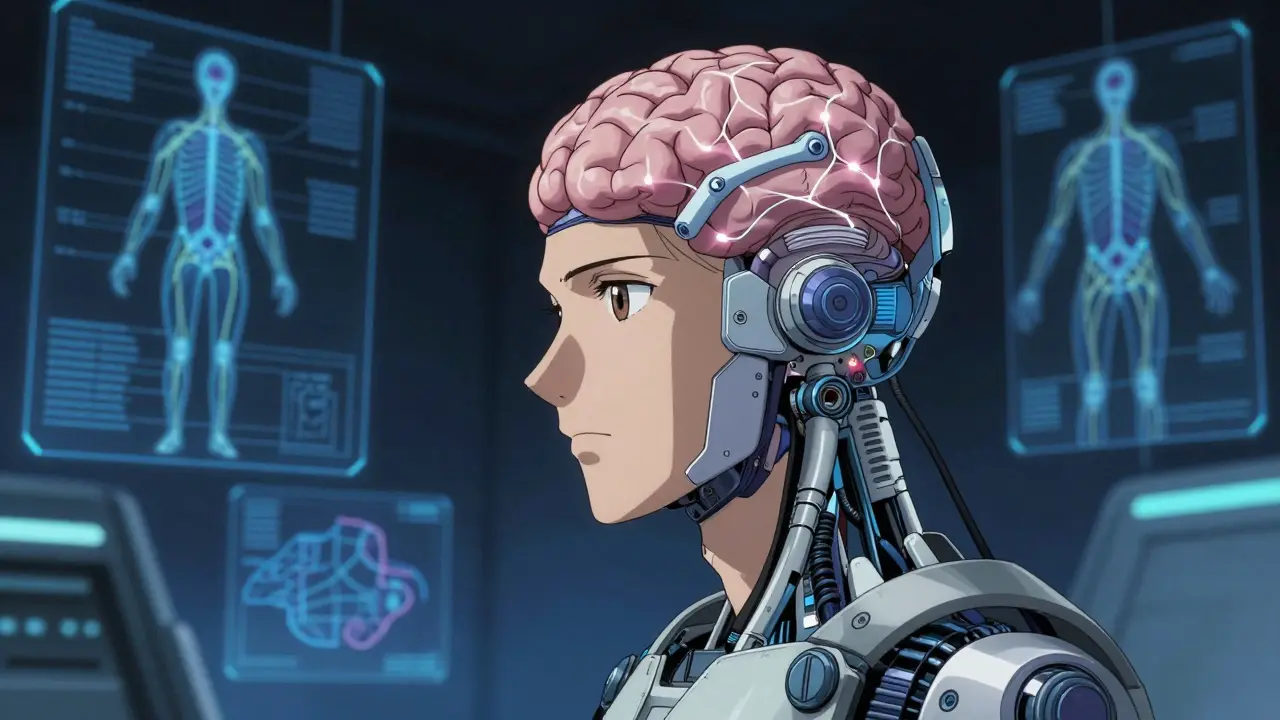
The Future of Neural Recovery
We are entering an era where the "permanent' part of permanent injury might be questioned. Brain-computer interfaces (BCI) are currently in trials, with some early data showing a 38% improvement in hand function for those with cervical injuries. Essentially, we are teaching computers to read brain signals and send them directly to robotic limbs or implanted electrodes, bypassing the damaged spinal cord entirely. Moreover, AI is starting to dictate therapy plans. Instead of a one-size-fits-all approach, centers are using data to personalize the intensity and type of exercise a patient receives. This precision medicine approach is likely to become the standard of care by 2026, ensuring that every minute spent in the gym is optimized for the specific injury level of the patient.Frequently Asked Questions
Can someone with a complete spinal cord injury ever walk again?
While the chances are statistically low-only about 1-3% of complete paraplegics regain ambulatory function-it is not impossible. However, most "walking" in complete cases is achieved through the use of advanced assistive devices like exoskeletons or extensive bracing rather than natural nerve regeneration.
How soon should rehabilitation start after an injury?
Rehabilitation should ideally begin within 24 to 72 hours after the patient is medically stabilized. Starting early is crucial to prevent secondary complications like muscle atrophy, joint contractures, and respiratory infections, which can permanently hinder the recovery process.
What is the difference between a complete and incomplete SCI?
A complete injury means there is no sensory or motor function preserved in the lowest sacral segments. An incomplete injury means some pathways remain intact, allowing some signals to pass through. Those with incomplete injuries generally have a much higher potential for functional recovery.
Do insurance companies typically cover robotic exoskeletons?
Coverage is unfortunately limited. Many insurance providers and Medicare only cover a portion of the costs for wheelchairs and specialized seating, often leaving patients with thousands of dollars in out-of-pocket expenses. Robotic exoskeletons are frequently viewed as "experimental' or 'luxury' by insurance, though this is slowly changing as more long-term data emerges.
How do I prevent pneumonia after a high-level spinal cord injury?
Respiratory interventions are critical. This includes using incentive spirometry, assisted coughing, and techniques like percussion and vibration. These interventions can reduce the incidence of pneumonia by up to 65% in patients with high cervical injuries.